
Laparoscopic Gastric Bypass
Laparoscopic gastric bypass combines restriction and malabsorption to give a powerful weight loss operation. The restrictive component is caused by creating a small pouch approximately 1/3 cup in size out of the top of the stomach. The malabsorptive component is due to a long segment of small bowel being excluded from where food travels down the GI tract, as nutrients no longer come into contact with the bypassed section of bowel they can not be absorbed and are passed out in your bowel motion. Gastric bypass operations cause significant hunger suppression and are very powerful in reversing diabetes as they have hormonal effects in addition to weight loss. There is no permanent removal of an organ so they are reversible if required (although extremely rare), additionally in some patients dumping syndrome may help deal with eating habits such as sugar addiction. Due to the malabsorptive nature of bypass operations they require frequent monitoring of nutrient levels with regular blood tests and vitamin tablets for the rest of your life. These issues need to be discussed with your surgeon in the appointments leading up to surgery to understand if bypass is right for you.
Roux-En-Y Bypass
Roux-en-Y bypass has remained an active part of the array of weight-loss operations since the 1970’s, as it is the gold standard treatment for GERD (gastro-esophageal reflux disease). This makes it an ideal procedure to treat both obesity and GERD with a single operation. It should be chosen for anyone who has been diagnosed with Barrett’s esophagus (chronic inflammation of the esophagus causing pre-cancerous cell changes). The technique is:
- The procedure is performed under general anaesthesia and takes approximately 2 hours.
- The patient is checked for a hiatus hernia and if one is present a repair is carried out.
- A calibration tube also called a bougie is inserted down the esophagus into the stomach to act as a guide ensuring the correct sized pouch is created.
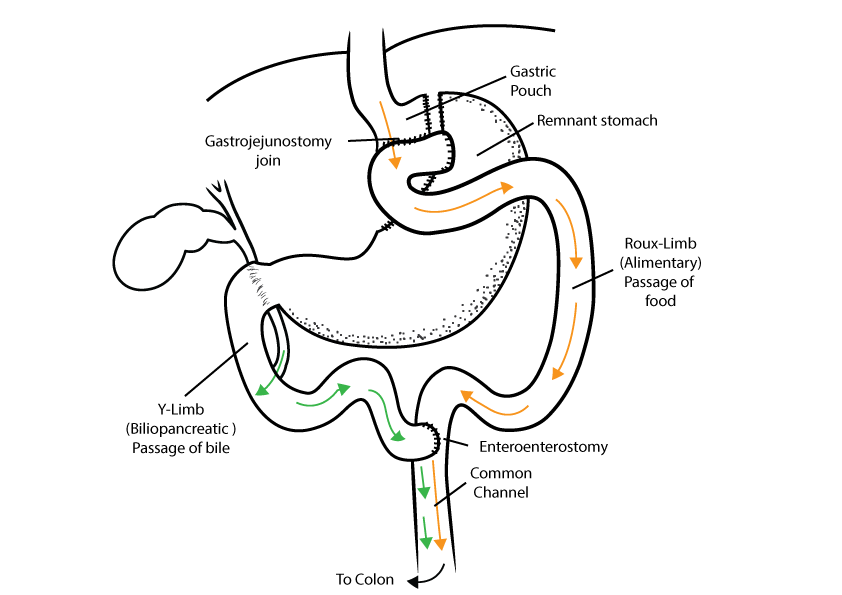
- A stapling and cutting device is used to create a small pouch out of the top of the stomach
- The start of the ileum (small bowel) is found and 60-120cm is counted off downstream from that location and at this point the small bowel is divided
- The distal end of the small bowel is brought up to the stomach and
a join is made between the side of the bowel wall and the end of the stomach pouch - The other end of the small bowel is joined back to the bowel again
100cm downstream from the stomach pouch.
Preparation For Surgery
- Routine blood panel: full blood count, kidney function, liver function, clotting factors, thyroid hormone, insulin, blood glucose, vitamins and minerals, cholesterol.
- Barium swallow test- to screen for GERD (gastro-esophageal reflux disease) and hiatus hernia.
- Upper abdominal ultrasound- to check liver size and presence of gallstones.
- Liver shrink diet- to reduce the volume of your liver so the surgery can be performed safely, this is a shakes based Very Low Calorie Diet such as Optifast, Optislim or KicStart, for most patients it ranges between 2-6 weeks depending on your BMI and liver size.
Post-Operative Diet & Recovery
- Shoulder tip gas pain is common after laparoscopic surgery and will subside within 48 hours, key-hole wounds should not be painful when managed with simple analgesia such as paracetamol.
- Nausea can be an issue in the days after surgery and you will be provided with a script for anti-emetics to allow adequate hydration.
- The first two weeks after surgery involve a liquid diet while the long wound in the stomach heals and swelling subsides.
- In weeks 3 and 4 a soft diet is consumed, these food stages allow comfortable progression back to solids at one month post-op.
- For those with desk jobs recovery time is usually 2 weeks before returning to work while those with physical jobs may need 3-4 weeks off.
- Exercise is built up gradually with short walks in week 3 after surgery, week 5 is the earliest for a cardio workout as you need to ensure you can consume enough calories, week 6 is the earliest for resistance training in order to avoid a hernia.
See our FAQ’s section for information regarding weight loss surgery.
